Childhood Adversity and Mental Health Outcomes
By Tara Keane

Tara Keane
I decided to study Health and Social Care as I wanted to change career after 20+ years. I left my job in retail 3 years ago and now work in Homeless Services. I enjoy the research modules, particularly quantitative research and also find psychology theories fascinating.
This is an example of my course work that I have submitted for module SSC223: Applied Quantitative Research in the Social Sciences.
Childhood Adversity and Mental Health Outcomes
Abstract
Introduction. It is only in recent years, that childhood adversities are being seen as predictors of mental ill health. A review of literature focussing on physical abuse and neglect and PTSD and depression was undertaken. Based on previous research significant associations between experiences of childhood physical abuse and neglect and diagnoses in adulthood of depression and PTSD were predicted Method For this analysis, a random sample of 25% of cases were generated from Wave 1 and Wave 2 National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) data (n = 8675). Crosstabulations and Chi Square Tests of Independence were run in RStudio to test the hypotheses. Findings There were significant associations found between childhood physical neglect and PTSD (X2 = 344.88, df=1, p<.05) and depression (X2 = 159.57, df=1, p<.05) and childhood physical abuse and PTSD (X2 = 372.086, df=1, p<.05) and Depression (X2 = 171.041, df=1, p<.05). Conclusion This research highlights that national policies need to address structural inequalities which cause childhood poverty which is associated with childhood neglect. It also highlights that practitioners who work with individuals with PTSD and depression should be aware that adverse childhood experiences may be at least part of the reason for such diagnosis.
LITERATURE REVIEW
It is only in recent years, that childhood adversities are being seen as predictors of mental ill health. These adversities are not exclusively focussed on neglect and abuse but also take into consideration other factors such as maternal mental health or loss of a parent (Read and Bentall, 2018). As mentioned in the introduction, Bowlbys Attachment Theory posits that an individuals experiences of relationships (through their caregiver) in childhood affect their development and their ability to form relationships in adulthood (Holmes, 2014). Developmental trauma is the term used to describe childhood trauma such as chronic abuse and neglect. If the caregiver is unable to ease the toxic stress caused by developmental trauma or if the caregiver is the cause of the toxic stress, it can lead to physical and mental ill health in adulthood. (Van der Kolk, 2005).
A review of literature focussing on physical abuse and neglect and PTSD and depression was undertaken. A study conducted by Sullivan and colleagues (2006), found that PTSD symptoms were correlated with forms of childhood abuse and neglect. The study showed that emotional abuse had a high association with PTSD and that sexual and physical neglect had a moderate association with PTSD.A further study carried out by Grasi-Oliveira and Stein (2008) found that childhood abuse and neglect predicted a high chance of PTSD and depression in later life. The study, which was carried out on patients in a public hospital seeking treatment, found that there was a history of physical abuse and neglect in childhood and because of these experiences, individuals were more vulnerable to PTSD and depression in adulthood. Other studies, such as one carried out by Widom (1999) agree that sexual and physical abuse are risk factors to PTSD in later life, however it did give not much attention to the impact physical neglect has.
Sexually abused women who also experienced physical abuse had a higher risk of developing PTSD. This was based on a study conducted by Roth and colleagues in 1997 who used an evaluation on participants in the DSM-IV PTSD Feld Trial.Further studies, such as one by Nothling and colleagues (2016) found that although trauma had an association with PTSD and depression, other factors such as community violence and demographics needed to be considered. Of the sample they surveyed they found that over half had symptoms of PTSD or depression but those who had experienced physical abuse alone made up just 5.3%. It found that the type of trauma experienced, rather than the trauma load predicted PTSD and depression. Other studies looking at depression and adverse childhood experiences, such as a study by Paterniti and colleagues (2017), found that physical neglect in childhood was a key predictor for depression in adulthood, and the effect of childhood physical neglect on the course of an individuals depression was independent of demographic variables. Studies in Taiwan by Cheng-Fang and colleagues, in 2008, found that 22% of those surveyed who had depression, had experienced childhood physical abuse and led the researchers to conclude that childhood physical abuse increased the risk of depression.
This research aims to answer the following research questions and to test their associated hypotheses.
Are those who experience physical neglect in childhood more likely to suffer PTSD in later life, than those who do not experience physical neglect?
Ho there is no association between childhood physical neglect and PTSD.
H1 there is an association between childhood physical neglect and PTSD in later life.
Are those who experience physical abuse in childhood more likely to suffer PTSD in later life, than those who do not experience physical abuse?
Ho there is no association between childhood physical abuse and PTSD in later life.
H1 there is an association between childhood physical abuse and PTSD in later life.
Are those who experience physical neglect in childhood more likely to suffer depression in later life, than those who do not experience physical neglect?
Ho there is no association between childhood physical neglect and depression in later life.
H1 there is an association between childhood physical neglect and depression in later life.
Are those who experience physical abuse in childhood more likely to suffer depression in later life, than those who do not experience physical abuse?
Ho there is no association between childhood physical abuse and depression in later life.
H1 there is an association between childhood physical abuse and depression in later life.
METHODOLOGY
This quantitative research took a post positivist approach. Karl Popper, a philosopher best known for his post positivist approaches, suggested that theories should be tested against data with the intention of falsifying hypotheses. (Fox, 2008). For the purpose of this research the Hypothetico-Deductive Method was used. This method identifies a broad problem, defines a statement about this problem, conducts literature review, defines research questions, and hypotheses, collects and analyses data and discusses the findings from the data. By deducting the observations, the hypotheses will be seen as true or false (Neuman, 2013).The ontological (philosophical framework) position of the research is critical realism. Critical realism is acknowledging the world is real, but acknowledging that its true workings may be beyond us. The epistemological (philosophical framework) position of the research is modified objectivism. Modified objectivism sees the world and researchers as separate but not independent.
METHOD
Sampling
The data is based on the 2001-2002 Wave 1 National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) and Wave 2 NESARC (2004-2005). It was conducted under the National Institute on Alcohol Abuse and Alcoholism (NIAAA)’s direction (NIAAA, 2010).
It should be noted, given the complex survey design, variance estimation procedures that assume a simple random sample are not appropriate. Given the clusters in the sample section, the variance estimates do not account appropriately for sample design effects and make non -significant differences appear significant. Taking this into consideration, all standard errors of estimate were generated using SUDAAN (Research Triangle Institute2008), a computer program that uses statistical techniques to adjust for sample design effects.
The sampling design and methodology of the NESARC can be found in “Source and Accuracy Statement for Wave 1 of the 2001 – 2002 National Epidemiologic Survey on Alcohol and Related Conditions” (Grant et al., 2003) and “Source and Accuracy Statement for the 2004 – 2005 Wave 2 National Epidemiologic Survey on Alcohol and Related Conditions” (Grant and Kaplan, 2005).
Participants
The sample set for Wave 1 was 43,093 individuals who were aged 18 and over from all fifty states and the District of Columbia, and included civilians, non-institutionalised adults and military personnel. The sample set for Wave 2 re-interviewed 34,653 of the original Wave 1 participants. Of the remaining 8,440, 3,134 were not eligible due to being institutionalised, on active duty, deceased, deported or mentally/physically impaired. The remaining 5,036 either refused or were unable to be located.
Response rates for Wave 1 was 81 percent and Wave 2 was 86.7 percent, yielding an overall response rate of 70.2 percent (NIAAA, 2010).
Variables
Age
Anyone over the age of 90 years of age was classed as 90 years of age (NESARC Codebook, 2008).
Sex
The code used was 1 for males and 2 for females. There were 42% males and 58% female. (NESARC Codebook, 2008).
Ethnicity
Ethnicity was measured with the codes 1 for White,non-Hispanic, 2 for Black,non-Hispanic, 3 for American Indian/Alaska Native, non-Hispanic, 4 for Asian/Native Hawaiian/Other Pacific Islander, non-Hispanic and 5 for Hispanic, any race. Participants were made up of 58.0% white, 19% black, 2% native, 3% Asian and 18% Hispanic (NESARC Codebook, 2008)
Perception of Current Health Status
Participants were asked to measure how the perceived their current health, the following options were given for this variable 1 as excellent, 2 as very good, 3 as good, 4 as fair, 5 as poor and 9 as missing data (NESARC Codebook, 2008).
Measures of Childhood Adversity
Physical Abuse
Participants were asked if they had experienced physical abuse before the age of 18 years old (NIAAA, 2010).
Physical Neglect
Participants were asked if they had experienced physical neglect before the age of 18 years old (NIAAA, 2010).
Measures of Mental Health in Adulthood
PTSD
Participants were asked if they had ever been diagnosed with PTSD by a health professional (NIAAA, 2010).
Depression
Participants were asked if they had ever been diagnosed with depression by a health professional. (NIAAA, 2010).
Analysis
For this analysis, a random sample of 25% of cases were generated. The initial dataset contained 8745 cases. Cases with missing data were omitted from the dataset in R Studio using na.omit function. This new dataset with cases with missing data point omitted contained 8675 cases. The minimum age was 20 and the maximum age was 90, 57% were female, 58% were white, 18.7% were black, 1.8% were native, 2.8% were Asian, and 18.6% were Hispanic. (RStudio, 2020).
FINDINGS
The age range for the sample was 20 to 90 years of age, with a mean of 49.2 (SD=17.25). The summary statistics for age are illustrated in Table 1.
Table 1. Descriptive Statistics for Age
|
Minimum |
Maximum |
Median |
Mean |
SD |
|
20.00 |
90.00 |
47.00 |
49.14 |
17.25
|
The distribution for age is illustrated below in figure 1.
Figure 1.
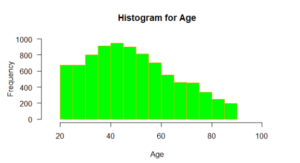
From Table 1 and Figure 1, shows that the distribution of age is positively skewed. When skewness was run in R Studio it was found to be 0.38, so although positively skewed it was within the normal range, so therefore the skewness would not be considered significantly skewed. The kurtosis at -0.68, although negative, would be considered mesokurtic (Hair et.al., 2017)
Boxplot for Age
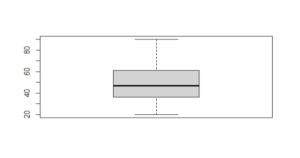 Figure 2.
Figure 2.
From Figure 2, the boxplot is comparatively short. The median age was 47 and corresponds to the thicker vertical line. The box shows the lower and upper quartiles of age (36-61) , while the whiskers show the ages below the 1st Quartile (20-36) and above the 3rd Quartile (61-90).
Table 2. Crosstabulation for Physical Neglect and PTSD (n=8675)
|
Physical Neglect |
PTSD (No) |
PTSD (Yes) |
|
|
|
|
|
|
|
|
|
Observed |
183 |
136 |
|
Expected |
284.5 |
34.5 |
|
% with PN |
57% |
43% |
|
% within Category |
2% |
15% |
|
|
|
|
|
Observed |
7555 |
801 |
|
Expected |
7453 |
902 |
|
% with no PN |
90% |
10% |
|
% within Category |
98% |
85% |
Table 3. Chi Square Test of Independence for Physical Neglect and PTSD
|
Chi Square |
Degree of Freedom |
P Value |
|
344.8854 |
1 |
<0.05 |
The results from the Chi Square suggest that the H0 can be rejected. These results indicate that those who experience childhood physical neglect are more likely to have a PTSD diagnosis than those who do not. Specifically, the results indicate that 43% of those who experienced childhood physical neglect, in contrast to 10% who did not experience childhood physical neglect met the threshold for PTSD.
Table 4. Crosstabulation for Physical Abuse and PTSD (n=8675)
|
Physical Abuse |
PTSD (No) |
PTSD (Yes) |
|
|
|
|
|
Observed |
199 |
147 |
|
Expected |
308.6 |
37.4 |
|
% with PA |
57% |
43% |
|
% within Category |
3% |
16% |
|
|
|
|
|
Observed |
7539 |
790 |
|
Expected |
7429.4 |
899.6 |
|
% with no PA |
91% |
9% |
|
% within Category |
97% |
84% |
Table 5. Chi Square Test of Independence for Physical Abuse and PTSD
|
Chi Square |
Degree of Freedom |
P Value |
|
372.0863 |
1 |
<0.05 |
The results from the Chi Square suggest that the H0 can be rejected. These results indicate that those who experience childhood physical abuse are more likely to have a PTSD diagnosis than those who do not. The results show that 43% of those who experienced childhood physical abuse, in contrast to 9% who did not experience childhood physical neglect met the threshold for PTSD.
Table 6. Crosstabulation for Physical Neglect and Depression (n=8675)
|
Physical Neglect |
Depression (No) |
Depression (Yes) |
|
|
|
|
|
Observed |
150 |
169 |
|
Expected |
244.2 |
74.7 |
|
% with PN |
47% |
53% |
|
% within Category |
2% |
8% |
|
Observed |
6493 |
1863 |
|
Expected |
6398.7 |
1957.2 |
|
% with no PN |
78% |
22% |
|
% within Category |
98% |
92% |
|
|
|
|
Table 7. Chi Square Test of Independence for Physical Neglect and Depression
|
Chi Square |
Degree of Freedom |
P Value |
|
159.5655 |
1 |
<0.05 |
The results from the Chi Square suggest that the H0 can be rejected. These results indicate that those who experience childhood physical neglect are more likely to have a diagnosis of depression than those who do not experience childhood physical neglect. The results indicate that only 2% of those who experienced childhood physical neglect did not experience depression, whereas 98% of those who had not experienced childhood physical neglect did not experience depression.
Table 8. Crosstabulation for Physical Abuse and Depression (n=8675)
|
Physical Abuse |
Depression (No) |
Depression (Yes) |
|
|
|
|
|
Observed |
164 |
182 |
|
Expected |
264.9 |
81.0 |
|
% with PA |
47% |
53% |
|
% within Category |
2% |
9% |
|
|
|
|
|
Observed |
6479 |
1850 |
|
Expected |
6378.0 |
1950.9 |
|
% with no PA |
78% |
22% |
|
% within Category |
98% |
91% |
Table 9. Chi Square Test of Independence for Physical Neglect and Depression
|
Chi Square |
Degree of Freedom |
P Value |
|
171.0412 |
1 |
<0.05 |
The results from the Chi Square suggest that the H0 can be rejected. These results indicate that those who experience childhood physical neglect are more likely to have a diagnosis of depression than those who do not experience childhood physical neglect. The results show that the expected amount for those with experience of childhood physical abuse is 81, however the observed results are over twice that at 182, showing an association between childhood physical abuse and depression.
DISCUSSION
The findings from the crosstabulations run can reject all four null hypotheses. The findings would agree with that of previous research, that show there is an association between childhood neglect and abuse and PTSD and depression in adulthood. The findings would suggest the need for interventions in childhood for those who have experienced physical abuse and neglect, as these adverse childhood experiences are key predictors of PTSD and depression. The findings in this research and other research would support this.
The limitations of the study are it was secondary data so questions specific to the research questions were not asked (frequency of exposure). The sample set was only 25% of the original data. The study was conducted in the US, so can only be generalized to the US population.
CONCLUSION
The findings concluded that physical abuse and neglect in childhood have an association with PTSD and depression in later life. These findings were conducted by running crosstabulations and chi square calculations on R Studio. The sample set was 25% of the original dataset and missing data was adjusted using na.omit in R Studio. Previous research was reviewed and the findings conducted for this research agreed with previous research that there is an association between the variables. This highlights that interventions need to take place for children as childhood neglect and abuse are predictors of PTSD and depression in later life. It also highlights the need for national policies to take into consideration such inequalities as poverty, as childhood neglect can often be the socio -economic environment a child lives in. It also highlights that practitioners who work with individuals with PTSD and depression should be aware that adverse childhood experiences may be at least part of the reason for such diagnosis. Therapy to address these issues should be considered along with medication to treat the symptoms of such diagnosis.
References
CDC-Kaiser Permanente Adverse Childhood Experiences (ACE) Study. (1995 to 1997). [online], Available: https://www.cdc.gov/violenceprevention/aces/about.html [Accessed: 01 January 2021]
Cheng-Fang, Y., Mei-Sang, Y., Cheng-Chih, C., Ming-Jen, Y., Ching, S., Mei-Hua, W., and Chu-Mei, L. (2008). Effects of childhood physical abuse on depression, problem drinking and perceived poor health status in adolescents living in rural Taiwan. Psychiatry and Clinical Neurosciences, 62 (5), pp.575-583. [online], Available: https://doi.org/10.1111/j.1440-1819.2008.01836.x [Accessed 7 January 2021].
Fox, N.J. (2008). Post-positivism. The sage encyclopaedia of qualitative research methods. London:Sage.
Grant, B.F.; Kaplan, K.D.; Shepard, J.; and Moore, T. (2003) Source and Accuracy Statement for Wave 1 of the 2001–2002 National Epidemiologic Survey on Alcohol and Related Conditions. Bethesda, MD: National Institute on Alcohol Abuse and Alcoholism.
Grant, B.F., and Kaplan, K.D. (2005). Source and Accuracy Statement for the 2004–2005 Wave 2 National Epidemiologic Survey on Alcohol and Related Conditions. Bethesda, MD: National Institute on Alcohol Abuse and Alcoholism.
Grassi-Oliveira, R. and Stein, L.M. (2008). Childhood maltreatment associated with PTSD and emotional distress in low-income adults. The burden of neglect. Elsevier.
Hair, J.F., Hult, G.T.M., Ringle, C.M., and Sarstedt, M. (2017). A Primer on Partial Least Squares Structural Equation Modelling. Sage.
Holmes, J. (2014). John Bowlby and Attachment Theory. United Kingdom: Taylor and Francis Ltd.
National Epidemiologic Survey on Alcohol and Related Conditions. Wave 2,2004-2005. Codebook. (2008).
Neuman, W.L. (2013). Social Research Methods. Pearson Education Limited.
NIAAA, (2010). Alcohol use and alcohol use disorders in the United States, a three year follow up: Main findings from the 2004-2005 wave 2 National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). US Alcohol Epidemiologic Data Reference Manual, 8 (2). [Online], Available: https://pubs.niaaa.nih.gov/publications/NESARC_DRM2/NESARC2DRM.htm#TOC15 [Accessed 18 October 2020]
Nothling, J., Sulliman, S., Martin, L., Simmons, C., and Serdat, S. (2016). Differences in abuse, neglect and exposure to community violence in adolescents with and without PTSD and depression. Journal of Interpersonal Violence.[online] https://doi.org/10.1177/0886260516674944 Accessed 06 January 2021 [Accessed 2 January 2021]
Paterniti, S., Sterner, I., Caldwell, C., and Bisserbe, J.C. (2017). Childhood neglect predicts the course of major depression in a tertiary care sample: a follow up study. BMC Psychiatry, 17 (113). [online], Available: https://doi.10.1186/s/2888-017-1270-x [Accessed 8 January 2021].
Read, J., and Bentall, R.P. (2018). Negative childhood experiences and mental health: theoretical, clinical and primary prevention implications. The British Journal of Psychiatry. 200 (2), pp.89-91. Cambridge University Press. [online], Available: https://doi.org/10.1192/bjp.bp.111.096727 [Accessed 2 January 2021]
RStudio Team (2020). RStudio: Integrated Development Environment for R. RStudio, PBC, Boston, MA URL http://www.rstudio.com/.
Roth, S., Newman, E., Pelcovitz, D., Van der Kolk, B., and Madel, F.S. (1997). Complex PTSD in victims exposed to sexual and physical abuse: results from the DSM-IV Field Trial for Posttraumatic stress disorder. Journal of Traumatic Stress. 10, pp.539-555. [online], Available: https://doi.org/10.1023/A:1024837617768 [Accessed 8 January 2021].
Sullivan, T.P., Fehon, D.C., Andres-Hyman, R.C., Lipschitz, D.S., Grilo, C.M. (2006). Differential Relationships of Childhood Abuse and Neglect subtypes to PTSD symptoms clusters among adolescent inpatients. Journal of Traumatic Stress 19 (2) pp. 229-239. [online], Available: https://doi.org/10.1002/jts.20092 [Accessed: 30 December 2020]
Van der Kolk, B.A. (2005). Developmental Trauma Disorder: Toward a rational diagnosis for children with complex trauma histories. Psychiatric Annals. 35 (5)
Widom, C.S. (1999). Posttraumatic stress disorder in abused and neglected children grown up. The American Journal of Psychiatry. 156 pp.1223-1229.